For millions of Indians managing heart conditions, a daily cocktail of prescribed medications is a common reality. Doctors often recommend combinations of drugs to control heart rate, manage blood pressure, and block excess calcium. While effective individually, a dangerous and potentially fatal medical emergency can arise if these drugs interact incorrectly under certain conditions. This condition is known as BRASH syndrome.
What Exactly is BRASH Syndrome?
BRASH is an acronym that describes a vicious cycle of interconnected health failures. According to Dr. Evan Levine, a board-certified cardiologist, it stands for: Bradycardia (dangerously slow heart rate), Renal failure (kidney dysfunction), AV nodal blockade (from heart-rate-slowing drugs), Shock (critically low blood pressure), and Hyperkalemia (elevated potassium in blood).
This syndrome typically strikes elderly patients with pre-existing heart disease. It begins subtly, often with something as simple as dehydration from vomiting, diarrhea, or a reduced fluid intake. For someone on AV node-blocking medications—like beta-blockers (metoprolol, bisoprolol), certain calcium channel blockers (verapamil, diltiazem), or digoxin—this minor stressor can spark a catastrophic chain reaction.

Reduced blood volume impairs kidney function. Weakened kidneys cannot properly filter potassium or clear the heart-slowing medications from the bloodstream. As both potassium and drug levels rise, they work in tandem to drastically slow the heart. This bradycardia then causes blood pressure to plummet, further reducing blood flow to the kidneys, which worsens their failure—creating the deadly "vicious circle" that defines BRASH.
Why BRASH is a Stealthy and Deadly Threat
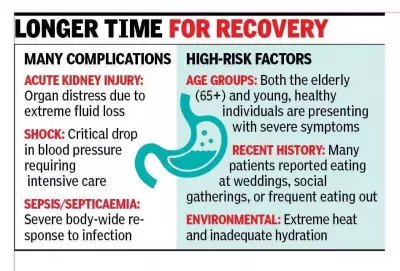
The extreme danger of BRASH syndrome lies in its deceptive presentation. Patients do not exhibit classic heart attack symptoms like chest pain. Instead, they may feel profound weakness, dizziness, confusion, and shortness of breath. A check reveals a very slow pulse and low blood pressure.
Critically, an ECG may not show the typical severe patterns of high potassium, making it easy for doctors to misdiagnose the situation as simple medication overdose or an unexplained slow heart rate. Standard emergency treatments for bradycardia, such as atropine or pacing, are often ineffective because they don't break the underlying cycle. If not recognized and treated specifically, the condition rapidly progresses to shock, multi-organ failure, and cardiac arrest.
Who is Most at Risk and How to Prevent It
The primary victims of BRASH are older adults with a history of heart disease and chronic kidney impairment, especially those with diabetes or long-standing hypertension. The risk multiplies if they are on one or more AV node-blocking drugs and experience dehydration, an infection, or use additional medications like NSAIDs (ibuprofen, naproxen) or potassium-affecting drugs (ACE inhibitors, ARBs).
Prevention hinges on awareness and vigilance. Patients and caregivers must:
- Know the list of AV node-blocking medications being taken.
- Seek immediate medical help for vomiting, diarrhea, or fever accompanied by dizziness and weakness.
- Avoid over-the-counter NSAID painkillers without consulting a doctor.
- Never self-adjust doses of heart or blood pressure medications.
- Ensure regular monitoring of kidney function and electrolyte levels through blood tests.
For clinicians, early detection is key. They must watch for the pattern of "disproportionate" bradycardia in patients on these drugs, especially when paired with even mild elevations in potassium (hyperkalemia) and creatinine. Recognizing this pattern early allows for targeted treatment that can reverse the syndrome and save lives.
Disclaimer: This information is for educational purposes only and is not a substitute for professional medical advice. Always consult your healthcare provider for diagnosis and treatment.